Read Full Article HerePrimer: Mustarde Cervicofacial Flaps
Large infraorbital defects present a challenge in recruiting sufficient tissue to reconstruct the wound while avoiding any downward traction on the inferior eyelid. In dermatology, the Mustarde cervicofacial flap, which is essentially a standard rotation flap with a few minor modifications, handily reconstructs most defects in this location and produces excellent cosmetic and functional results when carried out properly.
Anatomy
The Mustarde cervicofacial flap recruits skin laxity from the cheek and from the neck inferiorly. It is supplied by a pedicle developed to include the superficial cervical facia. While this flap has a random pattern blood supply, it has a broad base and intact blood supply from perforators of the facial artery. Venous drainage goes with gravity via the facial vein; therefore, venous and lymphatic drainage is excellent.
Design and Procedure
Initial flap design (Figure 1) is similar to a standard rotation flap, but with some important considerations and modifications. Initial study of the defect will lead the surgeon to determine if the incision should be carried out along the cosmetic boundary between the cheek and the inferolateral part of the orbit or if it should be carried laterally along the infraciliary border. The latter will more directly involve the lid margin, but it provides the benefit of reducing the risk of chronic lower lid edema when compared to incisions that interrupt the draining lymphatics along the full length of the orbit-cheek cosmetic boundary. Generally, if a defect is more laterally placed and does not require an incision along the full length of the orbit-cheek boundary, chronic lid edema does not result and an incision along this junction can permit execution of this closure with less morbidity for the patient related to bruising and swelling of the lid.
The incision begins at the superolateral part of the defect and courses superolaterally along either the infricilliary line or along the cheek-orbit boundary as the surgeon has determined. Next, once past the lateral canthus, the incision is carried superiorly into the temple to a peak height that is at least at or above the level of the lateral canthus. This deflection of the rotational arc superiorly in the temple is necessary to recruit additional tissue to support the lower lid and avoid downward traction and ectropion following completion of the closure that may be caused by flap shortening due to pivotal restraint as the flap is carried through its rotational motion. The incision traverses the temple in an arcing fashion before coursing inferiorly in the preauricular region approximately 5mm anterior to the junction between the ear and the cheek. This 5mm space is left to allow thicker skin of the preauricular cheek to bear the load of sutures when closing the secondary defect rather than using the comparatively weaker skin of the ear and tragus. The incision is often carried inferiorly to the level of the lobule for most applications in dermatology, but it can be extended onto the neck to develop additional motion. The incision onto the neck often courses in an arced fashion posteriorly in order to recruit additional tissue to close the preauricular region of the secondary defect.
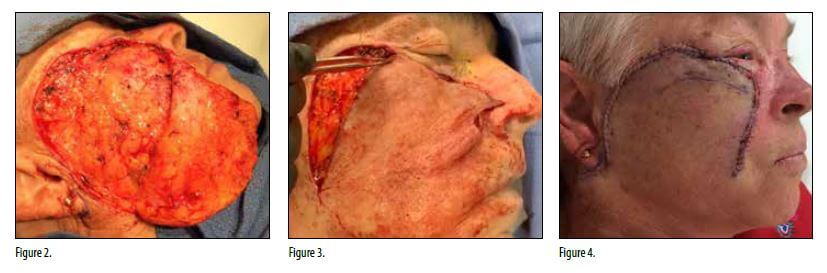
Once the incision is made, undermining is carried out to mobilize the flap. If an infraciliary approach is taken, undermining of the orbital skin is done below the dermis and above the orbicularis oculi muscle. On the temple where the incision is carried above the lateral canthus, undermining passes through the danger zone for the temporal branch of the facial nerve, so undermining here is done superficially immediately below the dermis as well to avoid injury to the nerve. Superficial undermining in this location also helps to better match the thickness of the skin in the recipient site below the eyelid. Once undermining is complete on the temporal and orbital skin, undermining is carried deeper to include the full thickness of the subcutaneous fat and the superficial musculo-aponeurotic system and platysma inferiorly (Figure 2). Undermining that is too thin (i.e. subdermal only) within the field of the flap over the cheek will increase the risk of distal flap necrosis. During undermining, it is helpful to pause and put the flap through its primary motion to ascertain where the standing cutaneous cone will fall as well as to assess for sufficiency of flap mobilization. When the position of the standing cone is determined, ensure complete undermining below and around the totality of the cone, particularly at the tip. Failure to undermine adequately in this location can cause significant and noticeable dimpling of the mid-cheek. In a properly designed flap, incision and undermining are generally complete when the flap can be laid over the primary defect and be in full contact with the lower lid portion of the defect before placing a single suture (Figure 3).
The Mustarde flap requires a suspension suture in most cases. Preferences vary with respect to choice of suture material with some surgeons preferring a clear polypropylene sutures while others utilize a strong absorbable suture, often of 4-0 size material. Positioning the periosteal suspension suture can be done by putting the flap into position over the primary defect and observing the part of the flap that is nearest the lateral orbital periosteum near Whitnall’s tubercle. The suspension suture is executed by taking a bite from the undersurface of the flap in the location described above and subsequently taking a bite to include the periosteum of the lateral orbital rim. One can confirm that the suture is in the periosteum by pausing then the needle is placed and gently rocking slightly back and forth with the needle driver grasping the needle. If the needle is holding periosteum, the patient’s head will move while performing this check. Complete this stitch by tightening a double-thrown knot sufficient to approximate the skin edges being careful not to overtighten and create a dimple in the flap. For defects involving the medial part of the lid as well, a suspension suture can be placed in similar fashion to either nasal periosteum or the medial canthal ligament. Once suspension sutures are placed, the remainder of the flap is closed with buried and superficial sutures in the standard fashion (Figure 4). The standing cone on the trailing side of the flap can be resolved by halves along the arc of the rotation, or a standing cutaneous cone can be excised below the lobule or above the pinna.
Conclusion
The Mustarde flap is a straightforward reconstruction utilizing the principles to basic rotation flaps with a few important modifications. Extending the incision superior to the lateral canthus in the temple, undermining adequately in the correct plane, and utilization of periosteal suspension sutures make this flap a reliable reconstruction for large infraorbital defects. l
 The incision begins at the superolateral part of the defect and courses superolaterally along either the infricilliary line or along the cheek-orbit boundary as the surgeon has determined. Next, once past the lateral canthus, the incision is carried superiorly into the temple to a peak height that is at least at or above the level of the lateral canthus. This deflection of the rotational arc superiorly in the temple is necessary to recruit additional tissue to support the lower lid and avoid downward traction and ectropion following completion of the closure that may be caused by flap shortening due to pivotal restraint as the flap is carried through its rotational motion. The incision traverses the temple in an arcing fashion before coursing inferiorly in the preauricular region approximately 5mm anterior to the junction between the ear and the cheek. This 5mm space is left to allow thicker skin of the preauricular cheek to bear the load of sutures when closing the secondary defect rather than using the comparatively weaker skin of the ear and tragus. The incision is often carried inferiorly to the level of the lobule for most applications in dermatology, but it can be extended onto the neck to develop additional motion. The incision onto the neck often courses in an arced fashion posteriorly in order to recruit additional tissue to close the preauricular region of the secondary defect.
The incision begins at the superolateral part of the defect and courses superolaterally along either the infricilliary line or along the cheek-orbit boundary as the surgeon has determined. Next, once past the lateral canthus, the incision is carried superiorly into the temple to a peak height that is at least at or above the level of the lateral canthus. This deflection of the rotational arc superiorly in the temple is necessary to recruit additional tissue to support the lower lid and avoid downward traction and ectropion following completion of the closure that may be caused by flap shortening due to pivotal restraint as the flap is carried through its rotational motion. The incision traverses the temple in an arcing fashion before coursing inferiorly in the preauricular region approximately 5mm anterior to the junction between the ear and the cheek. This 5mm space is left to allow thicker skin of the preauricular cheek to bear the load of sutures when closing the secondary defect rather than using the comparatively weaker skin of the ear and tragus. The incision is often carried inferiorly to the level of the lobule for most applications in dermatology, but it can be extended onto the neck to develop additional motion. The incision onto the neck often courses in an arced fashion posteriorly in order to recruit additional tissue to close the preauricular region of the secondary defect.